

CHOLERA (Cholera asiatica, Cholera indica), epidemic intestinal disease of Indian origin caused by infectious bacteria.
In Persian cholera was usually called wabā (wabāʾ), the term for any epidemic disease, but sometimes also hayża, which was more correctly applied to clinically similar but relatively benign diseases with which cholera was frequently confused before the German Robert Koch (1843-1910) discovered the bacterium (cholera vibrio, Vibrio comma, Vibrio cholerae Pacini 1854; Howard-Jones, p. 20) in 1301/1884, for example, Cholera sporadica (wabā-ye pāʾīza “autumn cholera,” ṯeql-e sard “sporadic cholera”) and infant diarrheas (Cholera ablactatorum; Schlimmer, pp. 130-35; Polak, I, p. 196, II, p. 345). In fact, it is possible to recognize the first clear appearance of the disease in Persia in the first great pandemic, which broke out in India in 1232/1817 and reached Persia in 1236/1821.
Epidemiological history (Macnamara; Khan, pp. 18-29). Persia, though located close to India, is protected from permanent endemic diseases of all kinds by the winter cold in the uplands. The study of the spread of cholera there is thus focused on the routes by which the disease entered the country: by sea through the ports on the Persian Gulf; overland from Afghanistan or Mesopotamia; and by land and sea, through the Russian empire and across the Caspian. Once it had arrived, it could spread over the Persian plateau by various routes.
The first pandemic initially arrived by sea, reaching Būšehr in Ramażān 1236/June 1821 and spreading from there to Dālakī, Kāzerūn, Shiraz, Ābāda, and Isfahan before being temporarily halted by the winter cold (Fraser, 1825, pp. 57-67). It reached Tabrīz only in Šawwāl and Ḏu’l-qaʿda/July and August of the following summer, having arrived overland from Mesopotamia and the Ottoman empire, no doubt carried by Persian troops fighting the Turks north of Lake Urmia, especially after their scattered retreat. Despite the institution of a kind of quarantine at Zanjān, the disease spread from there to the royal camp at Solṭānīya (Fraser, 1826, pp. 307, 316-18, 326), then to Gīlān, and finally to Baku, on 5 Moḥarram/22 September, and Astrakhan, where its progress along the western Caspian coast was arrested for the moment. It continued to spread eastward, however, reaching Tehran, where the principal outbreak occurred in Rajab 1238/April 1823 (Khan, p. 18), and from there spread to Mašhad and all the major cities on the plateau.
In contrast, the second pandemic spread to Persia via Afghanistan, arriving in Tehran in Rabīʿ II 1245/October 1829 and in Rašt at the end of the year, before spreading to Baku and Astrakhan, even reaching St. Petersburg in 1831. The first wave of the third pandemic followed the same route (reaching Mašhad in 1260/1844, Tehran and Tabrīz at the end of 1261/1845, and Isfahan in Šaʿbān 1262/August 1846). It affected mainly cities in the north; those in the south escaped almost entirely. The disease then spread to Baghdad in the west and to Tiflis and Astrakhan in the northwest. The route by which the second wave spread is more obscure; it lasted from 1267/1851 to 1279/1862, with a total of nine outbreaks (Khan, p. 23), five at Tabrīz and three at Tehran in ten years (Polak, II, p. 345; Issawi, p. 21). It was supposed by some early physicians to have arisen in the Russian cities along the Caspian, where the previous epidemic had not yet been extinguished (Khan, p. 23), but this idea was not generally accepted even at the time (Tholozan, pp. 42-43). In fact, during the eleven-year period in question the disease was rampant everywhere on the Persian plateau, breaking out suddenly at specific localities, for example, at Yazd in 1277-78/1860-61, without any identifiable provenience (Tholozan, pp. 39-40; see also Nāṭeq, pp. 16-17). As a result it was widely considered to be an endemic disease, a hypothesis energetically refuted by Joseph Désiré Tholozan, probably the best medical observer in Persia at that time; he insisted on the fundamentally healthy environment of the plateau (pp. 49-51).
As for the fourth pandemic, which raged in Persia from 1281/1865 to 1288/1871, there is no question that it arrived there from Mesopotamia and Turkish Kurdistan, spreading as far as the Caspian only in the final stages. In 1286/1869 Adrien Proust, the French pioneer of international cooperation on hygiene and father of Marcel Proust, paid an official visit to Russia and Persia; he disembarked at Anzalī but met the disease only at Qazvīn, on 21 Jomādā II/14 September (Khan, p. 24). The fifth pandemic, which thoroughly ravaged Persia in 1308-10/1891-92, seems to have arrived by two routes simultaneously: one from Herat via Mašhad, the other from Baṣra and Mesopotamia. The disease reached the shores of the Caspian in the winter of 1310/1892. The sixth, and last, pandemic, which originated in India in 1901 and reached the Persian Gulf ports (Bandar-e ʿAbbās, and Būšehr) in the same year, did not cross the southern Zagros or penetrate to the interior of the country. The second wave of the disease, in 1321/1903, was more serious, however. One source was Baṣra, whence it spread to Būšehr and as far as Shiraz; simultaneously the main route by which the infection reached the plateau was from Baghdad via Qaṣr-e Šīrīn, Kermānšāh, and Hamadān and thence to Tehran and Mašhad, on one hand, and Tabrīz and Azarbaijan, on the other.
From this extensive sequence of epidemics it is possible to extrapolate some general conclusions about the routes by which cholera reached Persia. It arrived three times via Afghanistan, three times overland from the west, only twice through the Persian Gulf (the second time without spreading to the plateau), and perhaps once across the Caspian. The land routes thus unquestionably predominated in the spread of the contagion, though it might reach Persia indirectly from the west as often as directly from the east. As physicians had already noted in the 13th/19th century (Tholozan, p. 51), the diffusion of cholera throughout Persia was usually quite slow, much slower than in Europe, reflecting the difficult means of communication and the extreme slowness with which caravans traveled in Persia at that period. The pace at which the disease spread was, however, clearly more rapid in southern Persia than in the north and northwest: 45 miles a day from Mašhad to Tehran and 37 miles from Tehran to Ḵᵛoy, compared to 70 miles a day from Tehran to Shiraz (Rigler, II, p. 445). This difference certainly resulted from different prevailing temperatures; the warmer climate in the south was more conducive to spread of the disease, whereas cold slowed its advance on the northern plateau.
Treatment and sanitary control. The first serious attempts to establish a policy of cholera prevention in Persia were made during the period of Nāṣer-al-Dīn Shah (r. 1264-1313/1848-96), particularly after his first trip to Europe in 1290/1873; they resulted from serious outbreaks of cholera in Persia in the 1240s/1860s, during which the disease reached almost endemic proportions (see above). In 1285/1868 the first public-health council (majles-e ḥefẓ al-ṣeḥḥa) was established (Nāṭeq, p. 28). Although it never actually functioned, sanitary officers were appointed in various cities; they forwarded to Tehran detailed reports on the history of the disease in the provinces, the projected publication of which (Tholozan, p. 55) unfortunately never took place. In 1286/1869 Tholozan, the first personal physician to the shah, submitted his Rapport à Sa Majesté le Châh sur l’état actuel de l’hygiène en Perse. Progrès à réaliser et moyens de les effectuer (lith. Tehran, Jomādā 1286/August 1869), in which he set forth the main steps to he taken (Tholozan, p. 6). The most important were the hygienic measures proposed, for example, an absolute ban on pilgrims’ traveling abroad or within Persia during periods of epidemic (p. 44). Quarantines were widely believed to be impracticable and ineffective, despite presentation of some arguments to the contrary at the third International Sanitary Conference at Constantinople in 1282-83/1866 (Howard-Jones, pp. 23-34; Elgood, pp. 518-19). Nevertheless, there were several proposals for integrating Persia into the international system for the sanitary defense of Europe (Zennaro, pp. 216-23).
The sanitary council, which was moribund except for vain periodic spurts of activity during epidemics, began to function seriously only after 1322/1904 (de Warzée, pp. 172-73). It was the establishment of a Pasteur institute in Tehran in 1339 = 1300 Š./1921 (Persia, p. 11) that first provided the conditions in which control of cholera became possible. Between that time and the Revolution of 1357-58 Š./1978-79 the disease made only sporadic and negligible appearances in Persia (1302 Š./1923, 1317-18 Š./1938-39, 1344 Š./1965, the last caused by a variant strain of the bacterium, vibrio El Tor (šebh-e wabā), named for the station at the southern tip of Sinai, on the Red Sea, where pilgrims to Mecca were formerly required to undergo quarantine (Howard-Jones, pp. 73, 82, 88); it arrived mainly from Afghanistan (Fischer, pp. 44-45), without ever reaching true epidemic proportions. In the 1360s/1980s, however, the arrival on Persian soil of almost 2 million Afghan refugees has caused a serious deterioration in health conditions. At Bīrjand, for example, twenty-seven cases were recorded in 1366 Š./1987 (data gathered by the author). It is probable that the disease is now nearly endemic in southern Khorasan.
Cholera in Persian life in the 13th/19th century. Before the disease was brought under control the ravages of cholera were severe in Persia. Although no precise statistical data are available, reliable observations attest the magnitude of the losses of human life. In 1236/1821 at Būšehr, though the majority of the population of about 10,000 fled the city at the first warning of the disease, there were nevertheless about 400 deaths, thirty to forty a day at the peak of the epidemic, with a maximum of forty-three in one day and an average of thirteen or fourteen a day over the entire period of the outbreak (Fraser, 1825, pp. 59, 65-66). At Shiraz, where the population was estimated at 35,000-40,000, there were eighty deaths on the first day of the epidemic and 200 on the third; the total was certainly as high as 5,000-6,000, that is, 12-15 percent of the population (Fraser, 1825, pp. 84, 95-96, 101). At Tabrīz, with a population that was “certainly not more than a hundred thousand,” the number of deaths is said to have reached 500 a day at the height of the epidemic in 1251/1835 (Burgess, p. 106). The total of deaths during the outbreak of 1262/1846 has been variously reported at 6,000 (Issawi, p. 20), 7,000-8,000 (Burgess, p. 106), and 10,000, that is, about one-seventh of the city’s population (Rigler, II, p. 444); there were probably 15,000-20,000 deaths in the province of Azarbaijan as a whole (Burgess, p. 93). In the same year the number of deaths at Tehran is said to have reached 7,000, that is, one tenth of the population, in seventy days (Rigler, II, p. 439). A French diplomat in Tehran, Count Joseph-Arthur de Gobineau, estimated in 1273/1856 that one-third of the city’s population had died during the summer (II, p. 234). At Tabrīz in 1279/1861 deaths totaled 2,487 (Issawi, p. 21). In only one of the twenty quarters of Shiraz the British physician C. J. Wills counted seventy-two corpses in one morning in 1286/1869 (p. 223). According to Ḥasan Amīn-al-Żarb an outbreak of cholera in 1288/1870 after a famine killed 200-400 in Tehran and 400-500 at Mašhad (Nāṭeq, pp. 17-18). The epidemic of 1310/1892 seems to have been equally murderous. Between 26 Moḥarram and 1 Ṣafar/20 and 25 August there were 800 deaths a day in Tehran (Feuvrier, p. 410), among a population already cut in half by the summer exodus. Eʿtemād-al-Salṭana estimated that deaths in Tehran totaled 23,000 (Nāṭeq, pp. 18-19). In the same year cholera killed 10,000 people in Gīlān (Issawi, p. 21).
It is thus possible to estimate that during the periodic waves of epidemic the large Persian cities suffered losses as high as 10-20 percent of their populations, a much higher proportion than was typical in large European cities at the same period (Bourdelais and Raulot, passim). Contemporary physicians were well aware of this fact; one of them noted in 1286/1869 that Persia was certainly one of the countries most ravaged by cholera in the preceding half-century (Tholozan, p. 30). In the 1390s/1870s the population of Hamadān impressed one foreign visitor as having been considerably reduced by the disease (Bassett, p. 131).
Losses from cholera were, however, very uneven throughout the country. For example, the relatively mild character of the epidemics at Isfahan was noted at the time and attributed to the fact that the domestic drains, which emptied directly into the streets, were cleared regularly and their contents carried to the fields for use as fertilizer. In addition, in the subsoil underlying the entire expanse of the city there was a shallow (3-5 m) but very pure aquifer fed by percolation from the Zāyandarūd, which ensured satisfactory drainage (Tholozan, p. 22). Cholera epidemics seem also to have been relatively mild in Gīlān (Rabino, p. 55). In the small towns (e.g., Langarūd, with thirty victims in twelve days in 1270/1854; Brugsch, II, p. 484) and especially in the countryside losses were fewer than in the large cities.
The reported number of deaths also tended to become inflated as rumors circulated among the public; according to the Dutch traveler T. Lycklama a Nyeholt (IV, p. 71), in Rabīʿ II 1284/August 1867 the eight or ten deaths a day in Tehran were reported in Hamadān as fifty deaths a day and farther west, at Ṣaḥna, as 100 a day. It is clear that in the 13th/19th century, before the development of programs for prevention, cholera profoundly affected popular beliefs, especially giving rise to entirely imaginary prophylactic measures. The Persians, like the Hindus, believed that the onset of cholera was signaled by the almost total disappearance of flies, supposedly in fear of the gigantic fly “Firaz,” which embodied the disease and, though invisible to human beings, was clearly visible to all insects. As she possessed the ability to fly with extraordinary rapidity, she could, if she wished, alight on every inhabitant of a large city in a single day. Whoever was brushed by her wings would immediately fall ill; those who touched her head would die, without hope of remedy (Cabanès, pp. 250, 252; cf. Massé, Croyances I, p. 206). People thus sought to protect their cities by means of various talismans and magic formulas (Massé, Croyances II, p. 330; Houtum-Schindler, p. 125; Wills, p. 290). Funerals posed particularly formidable problems and sometimes even led to serious disturbances. In 1310/1892 at Bījār, for example, because the cemeteries were located in town the dead had to be buried near a village in the country; the fearful villagers exhumed the corpses, however (Wilson, p. 159).
It is clear that cholera weighed heavily on the social atmosphere of large Persian cities during the greater part of the 13th/19th century. Traditional medicine was limited to combating the disease, deemed “hot,” with cold in the form of more or less icy baths. In the absence of any effective cure the only possible solution was flight to the mountains, considered to be almost immune to the disease at all seasons (Gobineau, I, p. 309). In fact the greatly increased popularity during the century of the traditional practice of seminomadism among city dwellers, who migrated in summer to the country and especially to high places, was largely attributable to fear of cholera. In 1310/1892 Nāṣer-al-Dīn Shah, who had arrived on 9 Moḥarram/15 August at his palace in Solṭānābād, left it hurriedly three days later, in order to take refuge at Šahrestānak, at an altitude of 2,500 m. Unfortunately, the disease, carried by members of his own court, took hold there and spread rapidly; there were fifty cases and twenty deaths in the royal camp and the neighboring village (Feuvrier, pp. 407-11). At mid-century the ladies of Tabrīz apparently even greeted the arrival of cholera epidemics with pleasure, as they provided the excuse to go into the mountains and lead a more agreeable and less isolated life (Sheil, p. 93).
Bibliography
J. Bassett, Persia, the Land of the Imams. A Narrative of Travel and Residence, 1871-1885, London, 1887.
P. Bourdelais and J.-Y. Raulot, Une peur bleue. Histoire du choléra en France, Paris, 1987.
H. Brugsch, Reise der königlichen preussischen Gesandtschaft nach Persien, 1860 and 1861, 2 vols., Leipzig, 1863.
C. and E. Burgess, Letters from Persia, Written by Charles and Edward Burgess, 1828-1855, ed. B. Schwartz, New York, 1942.
A. Cabanès, Mœurs intimes du passé V. Les fléaux de l’humanité, new ed., Paris, 1920.
C. Elgood, A Medical History of Persia and the Eastern Caliphate. The Development of Persian and Arabic Medical Sciences from the Earliest Times until the Year A.D. 1932, Cambridge, 1951; repr. Amsterdam, 1979.
J. Feuvrier, Trois ans à la cour de Perse, new ed., Paris, 1906.
L. Fischer, Afghanistan. Eine geographisch-medizinische Landeskunde, Berlin and Heidelberg, 1968.
J. B. Fraser, Narrative of a Journey into Khorasan in the Years 1821 and 1822, London, 1825.
Idem, Travels and Adventures in the Persian Provinces on the Southern Banks of the Caspian Sea, London, 1826.
J.-A. de Gobineau, Trois ans en Asie, 2 vols., Paris, 1859; repr., Paris, 1922.
M. Hekmat, Endemic Diseases of Iran, Ann Arbor, Mich., 1964.
A. Houtum-Schindler, Eastern Persian Irak, London, 1896.
N. Howard-Jones, The Scientific Background of the International Sanitary Conferences 1851-1938, Geneva, 1975.
C. Issawi, The Economic history of Iran 1800-1914, Chicago, 1971.
A. Khan, Choléra en Perse. Prophylaxie et traitement, Paris, 1908.
T. M. Lycklama à Nyeholt, Voyage en Russie, au Caucase, en Perse, etc. en 1866-68, 4 vols., Paris and Amsterdam, 1872-75.
C. Macnamara, A History of Asiatic Cholera, London, 1876.
H. Nāṭeq, “Taʾṯīr-e ejtemāʿī wa eqteṣādī-e bīmārī-e wabā dar dawra-ye Qājārīya,” in Moṣībat-e wabā wa balā-ye ḥokūmat, Tehran, 1358 Š./1979, pp. 9-45.
Persia, Oxford, 1945. J. E. Polak, Persien. Das Land und seine Bewohner, 2 vols., Leipzig, 1865.
A. Proust, Essai sur l’hygiène internationale, ses applications contre la peste, la fièvre jaune et le choléra asiatique, Paris, 1873.
H. L. Rabino, Les provinces caspiennes de la Perse. Le Guilân, Paris, 1917.
L. Rigler, Die Türkei und deren Bewohner in ihren naturhistorischen, physiologischen and pathologischen Verhältnissen, 2 vols., Vienna, 1852.
M. Sheil, Glimpses of Life and Manners in Persia, London, 1856.
J. D. Tholozan, Prophylaxie du choléra en Orient. L’hygiène et la réforme sanitaire en Perse, Paris, 1869.
D. de Warzée, Peeps into Persia, London, 1913.
C. J. Wills, In the Land of Lion and Sun, or Modern Persia, London, 1883; new ed., London, 1891.
S. G. Wilson, Persian Life and Customs, 3rd ed., New York, 1900.
S. Zennaro, Étude sur le choléra à l’occasion de l’épidémie de Constantinople en 1865, Constantinople (Istanbul), 1870.
(Xavier De Planhol)
The borrowed Arabic noun wabāʾ is used in Darī (Afghan Persian) and Pashto to denote all epidemic diseases, including cholera. For the sake of precision, the international term kōl(e)rā has been adopted in modern Afghan medical parlance.
Originally endemic in Bengal, cholera is transmitted mainly through ingestion of water, raw fruit, or vegetables that have been contaminated with the bacterium Vibrio cholerae (discovered by R. Koch 1843-1910). Its epidemic diffusion worldwide was made possible by the transport revolution, which immensely increased the geographical mobility of infected persons. The establishment of British rule in India was a significant factor in this process, which has been reflected in eight great pandemics since 1817. Afghanistan, with its close links to the Indian subcontinent, has been one of the hardest-hit regions; it also became a major relay station in the overland spread of cholera epidemics to countries farther west.
History. In the early years of the 19th century cholera appears to have been unknown in Afghanistan. Mountstuart Elphinstone (p. 140) did not list it among the country’s most common diseases in 1815. Afghanistan also escaped the first cholera pandemic (1232-35/1817-23), which spread from India mainly by sea (see i, above), but it bore the full brunt of the second pandemic (1241-53/1826-37). The earliest evidence is found in reports of cholera in the Kabul and Ḡaznī districts in 1242/1827 (Masson, I, pp. 188, 243). This crucial date marks the beginning of a succession of epidemics that swept over Afghanistan repeatedly until 1344 Š./1965.
A detailed history of the cholera epidemics in Afghanistan since 1242/1827 cannot now be pieced together. It is impossible even to say how many epidemics struck the country, because continuous documentation for the period before 1309 Š./1930 is lacking. Some observers have suggested an approximate ten-year frequency (Gazetteer of Afghanistan V, p. 155; Euan Smith, p. 33), but there are reasons to suppose that the rate was much higher. Between 1309 Š./1930 and 1344 Š./1965 no fewer than eight epidemics were recorded (1309 Š./1930, 1315 Š./1936, 1317-18 Š./1938-39, 1320 Š./1941, 1325 Š./1946, 1339 Š./1960, 1344 Š./1965), that is, an average of one every four years. In the 13th/19th century, when no sort of prophylaxis was practiced, the incidence of infection must have been still higher. For the period 1296-1321/1879-1903 it has been possible to identify epidemics at average intervals of three years (1296/1879, 1302/1885, 1306/1889, 1309-10/1891-92, 1317-18/1899-1900, 1320-21/1902-03); for the earlier period there is evidence that epidemics occurred in 1244/1829, 1255/1839, 1260-61/1844-45, 1278/1861, and 1284/1867 (MacNamara, pp. 83, 131, 148, 154, 265, 352), but this list cannot be taken as complete.
Not all the epidemics were equally virulent or widespread. One of the worst was undoubtedly that of 1310/1892, which was reported to have caused 100,000 deaths throughout the country, including 14,000 at Kabul, or about 10 percent of the city’s population at the time (IOR, L/P + S/7/66/1263 and 1676). On the other hand, that of 1296/1879 is said to have killed only 800 victims in the Lōgar district south of Kabul, that is, 2.5 percent of the district’s population (Euan Smith, p. 33), though it also struck many other districts for which no estimates are on record. The epidemic of 1302/1885 wiped out a quarter of the population of Qandahār, if the figure of 7,500 deaths counted in 105 days (IOR, L/P + S/7/45/1505) deserves credence; it does not seem at all improbable in view of the reported occurrence of hundreds of deaths every day in the same city at the height of the epidemic of 1261/1845 (Ferrier, pp. 366-67). In the absence of any statistics such simple estimates can be accepted as evidence that the mortality resulting from the great cholera epidemics of the 19th century was extremely high; they explain why the Afghans dreaded cholera much more than smallpox, the other great epidemic bane at that time (Thornton, p. 90). It must be added that people were not only completely ignorant of the treatment for cholera but also had no understanding of the most elementary rules of hygiene: At Kabul corpses were washed in the river from which the city drew its drinking water (Gray, p. 467; Martin, p. 45)—a practice still customary in rural areas at the time of the epidemic of 1339 Š./1960 (Planking et al., p. 20). The great speed of the disease’s spread, which impressed all observers, was owing to contamination of rivers and streams.
Mortality from cholera was particularly high when an epidemic struck in a year of food shortage, attacking bodies already weakened by undernutrition: for example, in southern Afghanistan in 1302/1885 (IOR, L/P + S/7/45/857) and at Kabul in 1320/1902 (Martin, pp. 55, 137).
To cope with these ordeals, the people had no expedient other than more or less orthodox religious rites. Communal prayers, processions of elephants carrying sacred relics, and sacrifices of animals were among the exercises marking peak periods of epidemics (IOR, L/P + S/64/1459; Martin, p. 86; Ferrier, p. 367). Only the ruling class could obtain a measure of protection, either by maintaining a sort of cordon sanitaire around their urban residences (Thornton, p. 90) or by hastily quitting the insalubrious capital for refuges in the nearby countryside, particularly Paḡmān, a mountain resort with a reputation for good water. During the great epidemic of 1309-10/1891-92, the amir ʿAbd-al-Raḥmān (1260-1319/1844-1901) lived a roving life for more than a year; he spent the early winter of 1309/1891 at Paḡmān (an unprecedented event), then stayed at Endakī (Čehel Sotūn) south of Kabul, then at Rešḵōr, and finally again at Paḡmān from Ramażān 1309/April 1892 until his return to Kabul in Rabīʿ II 1310/November 1892 (IOR, L/P + 5/7/64/1381 and 65/605; Gray, pp. 468-69, 493); he even posted guards along the Kabul-Paḡmān road to keep out traffic and thus the risk of infection (IOR, L/P + S/7/64/1383f.; Gray, p. 469).
In the 1310s Š./1930s there was a decisive turn for the better, owing to the establishment of some control of the frontiers, isolation of centers of infection, and, above all, massive vaccination campaigns. The vaccines used in the first campaign, in 1309 Š./1930, were imported from the U.S.S.R. and India (R. R. Maconachie, British ambassador to Kabul, Annual Report 1930, IOR, p. 24). Local production of anticholera vaccine was started in 1317 Š./1938 (W. K. Fraser-Tytler, British ambassador to Kabul, Annual Report 1938, IOR, p. 36), and the number of people vaccinated in that year totaled about a half-million, 40 percent of them at Kabul (Jusatz, p. 262). A special vaccine-production unit (Moʾassasa-ye waksīnsāzī) was opened at Kabul in 1335 Š./1956 (Fischer, 1968, p. 92); its output was sufficient to permit the vaccination of some 3 million people during the epidemic of 1339 Š./1960 (Ministry of Planning, 1963, p. 48) and 1,570,000 during that of 1344 Š./1966 (idem, 1965, p. 38).
Despite the scarcity of medical services and the weakness of governmental administration, the public-health policy launched in the 1310s Š./1930s yielded very positive results. For the first time waves of epidemic were reported to have been halted along the frontier without breaking into Afghanistan, for instance, in 1314 Š./1935 (W. K. Fraser-Tytler, Annual Report 1935, IOR, p. 24), in 1326 Š./1947 (Ministry of Public Health, p. 9), and in 1349 Š./1970. Furthermore, those epidemics that did penetrate into Afghanistan were less extensive and less disastrous than those of the 13th/19th century. Only 3,855 cases of cholera were recorded in 1317 Š./1938, 1,444 in 1318 Š./1939, 889 in 1339 Š./1960, and 1,564 in 1344 Š./1965. Epidemics were successfully confined to the frontier districts of Paktīā and Nangrahār in 1315 Š./1936, 1320 Š./1941, and 1325 Š./1946. At the same time increasingly effective methods of cholera treatment were introduced, and they led to an impressive drop in the mortality rate, from 55.5 percent of known cases in 1317 Š./1938 and 57.8 percent in 1318 Š./1939 to 22.4 percent in 1339 Š./1960 and 20.8 percent in 1344 Š./1965 (Fischer, 1968, pp. 109-10). A. H. Abou-Gareeb (pp. 123, 126) reported even lower rates for the last two epidemics: 19.2 percent in 1339 Š./1960 (cf. Heine, p. 34: 17.5 percent) and 15.4 percent in 1344 Š./1965. These successes, however, remained fragile and unequally distributed, as shown by the range of mortality rates in districts during the 1339 Š./1960 epidemic: from 14.2 percent in Nangrahār to 36.4 percent in Qaṭaḡan, in general reflecting the unequal distribution of medical services on Afghan territory. On the other hand, the fragility of these successes is clear from the fact that, though only isolated cholera cases were recorded between 1344 Š./1965 and 1357 Š./1978 (Feachem, p. 8), a definite recrudescence of the disease became apparent in the 1360s Š./1980s. For the first time in twenty-two years, several fatal cases were recorded in 1366 Š./1987 (van Straaten, p. 14). They can be explained as one result of the general deterioration of health services and infrastructure in Afghanistan after the start of the civil war and Soviet occupation. For example the manufacture of anticholera vaccine virtually ceased, reportedly dropping from 96,500 ml in 1357 Š./1978-79 to 20,000 ml in 1359 Š./1980-81 and 2,000 ml in 1362 Š./1983-84, the lowest level since 1335 Š./1956 (Afghan statistical yearbooks for the years in question; 1 ml is the normal vaccination dose). Conditions in Afghanistan at the time of writing indicate that cholera has become a real threat to its people once again.
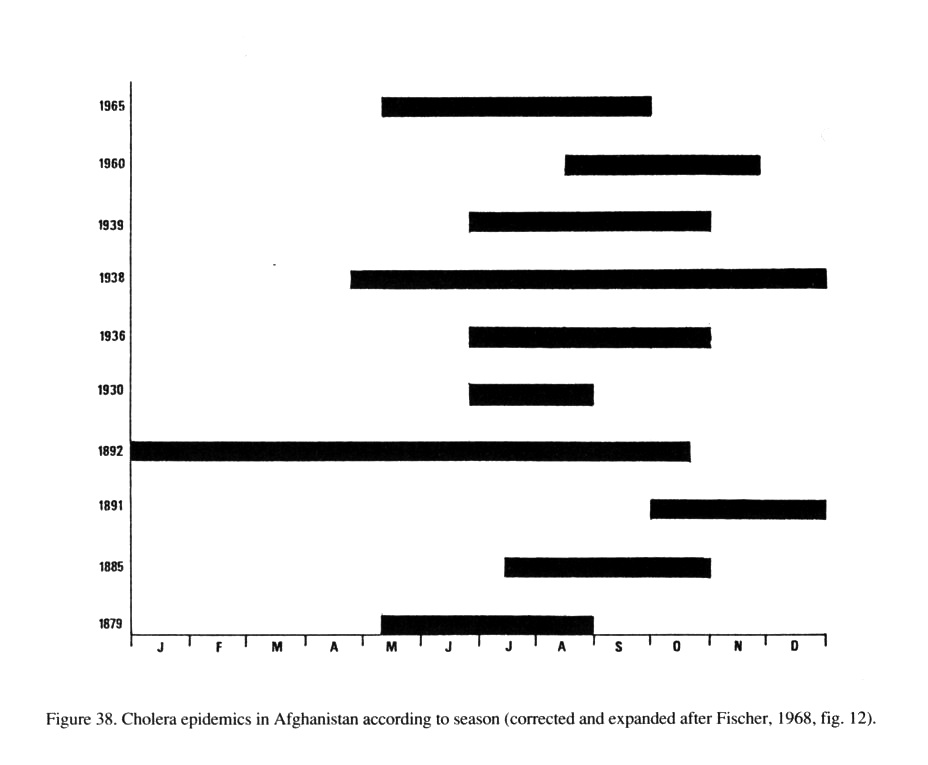
Epidemiology. In the subtropical and dry continental environment of Afghanistan cholera is more subject to climatic constraints than in humid tropical regions. Seasonal incidence has therefore been a distinctive feature of the epidemics in the country. Heat and humidity are the conditions most favorable to survival of the vibrio outside the human body. In Afghanistan, where heat and humidity never coincide, heat has proved to be the prevalent factor. Cholera in Afghanistan is primarily a disease of the hot, dry summer season, for the intense cold of the winter normally brings the activity of the vibrio to an end (see Figure 38). Nevertheless, the latter can survive in a dormant state during abnormally mild winters, as appears to have happened in 1309-10/1891-92 and 1317-18 Š./1938-39. After having been brought into Afghanistan through Peshawar at the end of April 1938, cholera swept through the entire southern part of the country until December; a lull of six months followed, and then the epidemic reemerged with even greater virulence, in June 1939, spreading from the middle Helmand, where the vibrio had hibernated during the winter (Fischer, 1968, p. 109). Even more convincing is the evidence of the epidemic of 1309-10/1891-92, when the winter brought about no significant abatement in the disease at all: After having been imported into Qandahār and Jalālābād almost simultaneously in the early autumn of 1309/1891 it spread to Kabul in November and Kōhestān in December, returned to Kabul in full force during January 1892, and finally reached Herat on 21 February (IOR, L/P + S/7/64 and 65, passim). Such occurrences arose in exceptional circumstances, however, and produced no lasting effect: Cholera never became endemic in Afghanistan. It has always been imported from abroad, almost always from India but at least once, in 1260/1844, from Bukhara (MacNamara, pp. 148-09),
{kind=link}
As for the identity of the carriers who imported and spread cholera in Afghanistan, most authors blame Pashtun nomads who, at least until 1358 Š./1979, used to spend the winters in the infested Indus lowlands (e.g., Fischer, 1969, pp. 136ff.). If they were correct, then the outbreaks should have coincided with the migration calendar and would have been concentrated in the spring (April-May), when the nomads return to their summer quarters. In fact, however, they did not coincide. Of nine epidemics for which there is sufficient information to permit comparisons (Figure 38) only three began in the spring, whereas five began in summer (June-August) and one in early autumn (end of September). The disease was clearly active throughout the entire warm half of the year. Nor is there any proof that the spring outbreaks were always caused by nomads. In 1317 Š./1938 cholera was apparently brought by Afghan pilgrims returning from the kumbh mela at Hardwar in Uttar Pradesh, India (W. K. Fraser-Tytler, Annual Report 1938, IOR, pp. 25-26; see also Pollitzer, pp. 83ff.); in 1344 Š./1965 it was probably brought by a pilgrim who had returned to the oasis of Andḵūy after being infected with the El Tor vibrio at Mecca (Abou-Gareeb, p. 125). These examples are evidence of the importance of the great Muslim and Hindu pilgrimages in spreading cholera—a point emphasized by many writers (most recently Pollitzer, pp. 927ff.). Another consideration is that cholera epidemics in Afghanistan always spread along the great caravan highways, rather than along the migration routes of the pastoral nomads, who have traditionally avoided the highways. The main channels for importation of the disease have been the Peshawar-Kabul and Quetta-Qandahār highways, which are apparently of equal importance in this respect. The perimeter route Kabul-Qandahār-Herat-Balḵ-Čārīkār, in particular its busiest stretch, between Kabul and Qandahār, has served as the main channel of diffusion within the country and also of transmission to neighboring Persia and Central Asia. The main relay stations have been caravansaries and, above all, market towns, where people converge and commingle.
{kind=link}
As nomads are scattered geographically, they could hardly have been responsible for the massive diffusion of an infectious disease. Traders and haulers (some, but not all, of nomadic tribal origin) were the main agents of cholera propagation in Afghanistan in the past.
References to unpublished archival sources in the India Office Records, London (IOR), are given in the text. A. H. Abou-Gareeb, “The 1965 Cholera Outbreak in Afghanistan,” Journal of Tropical Medicine and Hygiene 70/5, 1967, pp. 123-32.
M. Elphinstone, An Account of the Kingdom of Caubul and Its Dependencies, London, 1815; repr. Graz, 1969.
C. B. Euan Smith, Report on the Occupation of the Logar Valley from April to August 1880, Calcutta, 1881.
R. G. Feachem, Water- and Excreta-Related Disease in Afghanistan (roneo), Kabul, 1978.
J. P. Ferrier, Caravan Journeys and Wanderings in Persia, Afghanistan, Turkistan, and Beloochistan, London, 1857; repr. Westmead, Eng., 1971, and Karachi, 1976.
L. Fischer, Afghanistan. A Geomedical Monograph, Berlin and Heidelberg, 1968.
Idem, “Nomaden und Tropenkrankheiten,” in Nomadismus als Entwicklungsproblem, Bochumer Schriften zur Entwicklungsforschung and Entwicklungspolitik 5, Bielefeld, Ger., 1969, pp. 131-43.
J. A. Gray, At the Court of the Amir, London, 1895.
H.-D. Heine, Die Cholera im Mittleren Osten, Ph.D. diss., Tübingen, 1964.
H. J. Jusatz, “150 Jahre pandemische Ausbreitung der asiatischen Cholera von 1831 bis 1981,” Zentralblatt für Bakteriologie, Mikrobiologie und Hygiene A, 252, 1982, pp. 257-67.
C. MacNamara, A History of Asiatic Cholera, London, 1876.
F. A. Martin, Under the Absolute Amir, London and New York, 1907.
C. Masson, Narrative of Various Journeys in Balochistan, Afghanistan, and the Panjab, 3 vols., London, 1842; repr. Karachi, 1974, and Graz, 1975.
Ministry of Planning, Survey of Progress 1961-62, Kabul, 1963.
Idem, Survey of Progress 1965-66, Kabul, 1966.
Ministry of Public Health, Fifty Years of Health Development Program in Afghanistan, Kabul, 1968.
Z. A. Plankina et al., “Bor’ba s kholeroĭ v Afganistane,” Zhurnal mikrobiologii, èpidemiologii i immunobiologii 32/12, 1961, pp. 20-24.
R. Pollitzer, Le choléra, Geneva, 1960.
F. van Straaten, “The Health of a Nation,” Afghanistan (London) 9, 1988, pp. 13-14.
E. and A. Thornton, Leaves from an Afghan Scrapbook, London, 1910.
On the protection measures taken by the British army during its occupation of eastern Afghanistan during the cholera epidemic of 1879 see W. Trousdale, ed., The Gordon Creeds in Afghanistan, Putney, Eng., 1984, esp. pp. 29, 37.